Practice of Medicine
article
Reducing the Risks of Spinal Injury
Spinal injury and disease accounts for 3% of medical malpractice claims among emergency medicine doctors insured by MagMutual. In fact, spinal injuries are often among the most serious; 39.5% of patients become paraplegic and 59.9% quadriplegic.1
To help emergency medicine physicians reduce that number, MagMutual’s medical faculty and risk consultants have analyzed our claims data, determined the main causes of claims related to spinal injuries and developed strategies to improve patient outcomes.
Top Risks
The main causes of claims related to spinal injuries are:
- Failure to include/rule out spinal epidural abscess in differential diagnosis
- Failure to order the appropriate level MRI
- Communication issues
- Failure to sign out to oncoming Hospitalist with Outstanding Tests
Top Strategies for Reduction
Based on these top risk drivers, implementing the following clinical and operational strategies can help you prevent unexpected outcomes and increase defensibility of a medical malpractice claim:
Clinical strategies
- Thoroughly examine any patient with back pain who has fever, night sweats, numbness, weakness, incontinence, gait abnormalities or history of recent infection (cellulitis, abscess, urinary tract infection), IV drug use, chronic catheters, immunocompromised state or history of TB. Ask about urinary overflow incontinence (distended bladder or US showing retention) and fecal incontinence. A careful cardiac examination may show signs of a murmur suggestive of associated endocarditis. It is important to palpate each individual vertebra.
- Always develop a broad differential diagnosis, especially in patients with back pain, when it is easy to attribute the pain to a musculoskeletal cause. This is especially true if unexplained or ongoing fever, repeat visits to providers and pain out of proportion to the expected. Consider obtaining ESR and CRP in cases in which you are concerned about epidural abscess. While non-specific, the ESR and CRP are elevated in nearly all cases of epidural abscess. If unable to get radiologic studies (MRI), consider transferring to an appropriate facility, in a timely manner especially if elevated ESR or CRP. Consult a spine specialist for any patient for whom you have not sufficiently ruled out acute spinal emergency.
- Maintain a low threshold to refer to a specialist (orthopedics, neurosurgery, infectious disease), particularly if initial studies are normal and patient is still symptomatic, and/or consider obtaining definitive spine imaging, such as MRI. IV Drug Users (IVDU) warrant a heightened concern for infection, including endocarditis with associated epidural abscess.
Operational strategies
- Document expanded differential diagnosis, as well as decision making regarding testing (especially if taking a stepwise diagnostic approach that defers initial workup).
- Consider obtaining laboratory testing, including ESR and CRP. CT of the spine is extraordinarily poor at picking up spinal epidural abscess and shouldn't be relied upon. If suspicious enough to MRI the spine, include all levels because of a tendency for skipping lesions and multiple levels of involvement, up to nearly 20% of cases in some studies. Also, make sure the MRI is done emergently. While CT is a highly inaccurate test for pyogenic infections of the spine, complete spine MRI imaging should be ordered if a CT indicates any vertebral osteomyelitis or paravertebral abscess, because SEA is very often coincident with other infections. Not all blood cultures growing staph or strep are contaminants. Establish strict guidelines on blood culture follow-up.
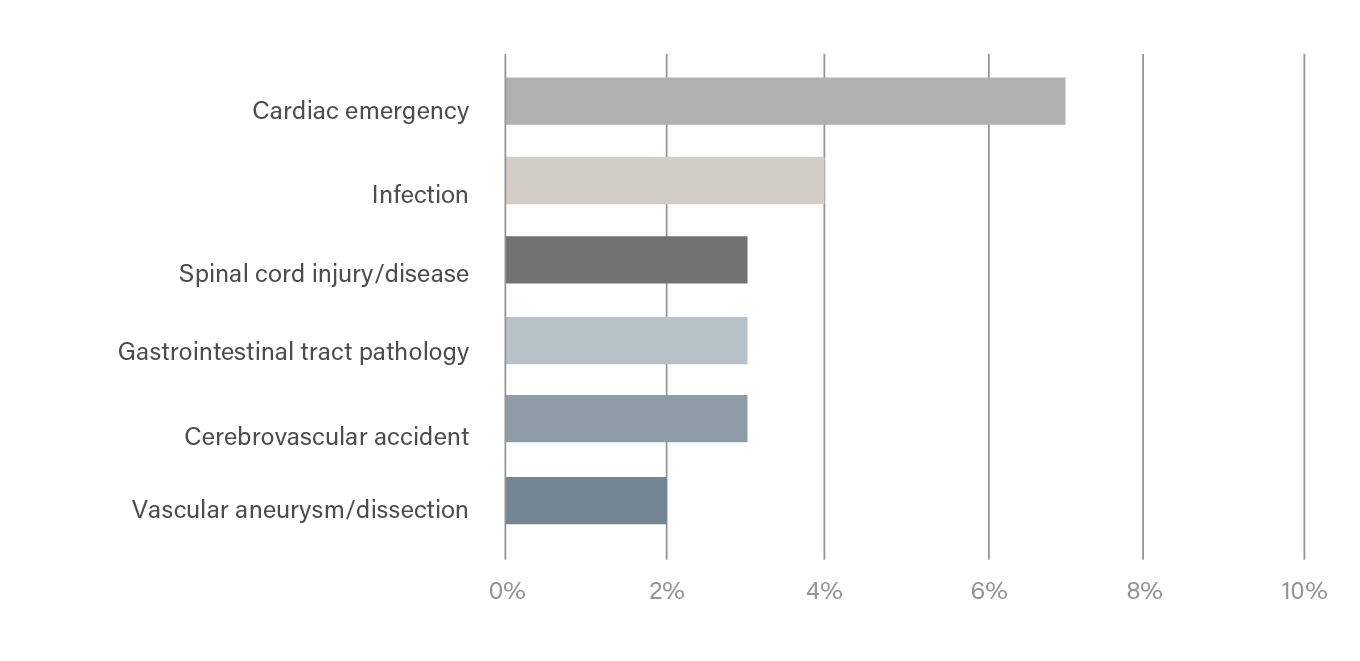
Other Top Risks
Though spinal injury accounts for most claims among emergency medicine according to our data, we’ve identified several other drivers of loss based on claims frequency, and severity:
Risk Drivers by Top Cause
| Key Loss Driver | Top Clinical Loss Cause | Top Non-Clinical Contributing Factor | % of Claims |
|---|---|---|---|
| (A) Cardiac Emergency | Diagnostic | Documentation | 7% |
| (B) Infection | Treatment | Documentation | 4% |
| (C) Spinal cord injury/disease | Diagnostic | Documentation | 3% |
| (D) Gastrointestinal tract pathology | Diagnostic | Documentation | 3% |
| (E) Cerebrovascular accident | Treatment | Communication | 3% |
| (F) Vascular aneurysm/dissection | Diagnostic | Documentation | 2% |
Risk Drivers by Frequency
Download the full report with strategies to help you reduce risk in all key areas that drive claims
MagMutual PolicyOwners: Log in to view the full report
Not a policyholder? Download Here
Data Collection & Methodology
Data is based on MagMutual closed claims data from 2011-2021 and corresponding exposure data. Clinical and non-clinical loss drivers are based on an in-depth review of each claim by a medical professional or clinical risk consultant. Risk reduction strategies are based on input from practicing physicians.
1 Source: https://www.sci-info-pages.com/spinal-cord-injury-facts-and-statistics/
02/24
Disclaimer
The information provided in this resource does not constitute legal, medical or any other professional advice, nor does it establish a standard of care. This resource has been created as an aid to you in your practice. The ultimate decision on how to use the information provided rests solely with you, the PolicyOwner.